Cognitive Overload in Clinicians: How to Prioritize Under Pressure
School-based and small-practice clinicians wear 27 hats on a good day. On the tougher days, it can feel like all 27 are slipping off your head while someone knocks on your office door asking if you’ve got “just a minute.” Meanwhile, your inbox behaves like it has something to prove.
A broken FM system? ASAP.
Upset patient waiting at your door before the office even opens? ASAP.
Parent question before you’ve even opened the chart? Apparently ASAP, too.
When everything is loud at the same time, your brain starts playing referee between tasks. All of whom insist that they matter most. Clinical training prepares us for diagnostics, treatment planning, and ethical reasoning. It doesn’t prepare anyone for the mental load of constant triage in environments that shift every 10 minutes.
Research confirms what we already know: Frequent interruptions and task switching increase stress and cognitive strain (Baethge & Rigotti, 2013; Rivera-Rodriguez & Karsh, 2010). When your cognitive capacity is stretched thin, everything blends together until decision fatigue takes over, and before you know it, your day starts running you instead of the other way around.
You need a framework that fits the reality of clinical work, not one designed for quiet offices that don’t exist.
The Eisenhower Model For Clinicians
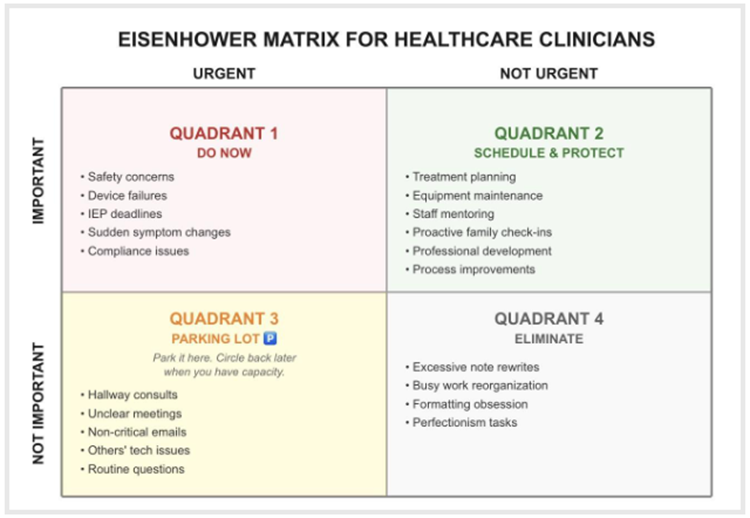
The Eisenhower model does something simple but powerful: It separates “urgent” from “important” (Covey, 1989). Not all urgent tasks are important, and not all important tasks are urgent. In clinical settings, urgency gets distorted by the sheer number of voices, needs, and systems competing for attention. A teacher’s crisis, a family’s worry, an admin request, a malfunctioning device...they all arrive with the same emotional weight. This model cuts through that noise by breaking your workload into four categories:
- Quadrant 1: Urgent + Important
- Quadrant 2: Important + Not Urgent
- Quadrant 3: Urgent + Not Important
- Quadrant 4: Not Urgent + Not Important
Let’s examine each quadrant.
Quadrant 1: Urgent + Important
This first quadrant falls into the “must handle now” category. There’s a real consequence if the action is delayed: safety issues, device failures affecting access, non-negotiable IEP deadlines, sudden changes in hearing or communication, compliance-driven supervision.
Clinicians manage this quadrant instinctively. But the problems start when your entire day creeps into Quadrant 1. When that happens, burnout risk increases, and recovery time shrinks (Maslach & Leiter, 2016). You can’t sustain a schedule built entirely on crises.
Quadrant 2: Important + Not Urgent
This quadrant keeps your work sustainable. It’s the planning your sessions, reviewing data, adjusting treatment plans, maintaining equipment logs, mentoring support staff, refining processes, checking in with families proactively.
This is the quadrant most likely to be neglected when your schedule gets tight, even though it actually can help prevent many Quadrant 1 emergencies. Quadrant 2 is the quiet foundation of good practice. Without it, you’re perpetually firefighting.
Quadrant 3: Urgent + Not Important
This is the sneaky one. It feels urgent because someone else wants attention now, but the outcome doesn’t actually change if it’s handled later: hallway consults, unclear meetings, non-critical emails, tech issues outside your role.
Quadrant 3 steals massive amounts of time. Even brief disruptions carry high cognitive costs, and regaining focus takes longer than the interruption itself; then, repeated disruptions compound fatigue across the day (Baethge & Rigotti, 2013; Rivera-Rodriguez & Karsh, 2010).
Quadrant 4: Not Urgent + Not Important
This quadrant consists of tasks that don’t move anything forward: reworking notes repeatedly, reorganizing materials because it feels productive, obsessing over minor documentation tasks like formatting. Often, Quadrant 4 tasks are coping behaviors that you tap into when your brain is tired. They’re not harmful, but they're not exactly helping, either.
How To Actually Use This Model
Here’s what the Eisenhower model looks like in practice:
Tuesday morning in a small audiology practice. Before your first patient, someone walks in with a broken hearing aid and looks panicked. Your brain tags it: Quadrant 1—device failure affecting access. You address it immediately.
While troubleshooting, a detailed insurance question comes through email. You mentally file it as Quadrant 3—urgent to them, not time-sensitive for you. You flag it to handle after morning appointments.
A reminder pops up: Your re-calibration log is due at the end of the month. You tag it: Quadrant 2—important but not urgent. You block 30 minutes on Friday afternoon to complete it before it becomes Quadrant 1.
Your next appointment arrives early wanting to “talk through a few concerns.” You assess: routine questions or new symptoms? If routine, Quadrant 3. You acknowledge them warmly and say, “Let me finish prepping, and I’ll give you my full attention in 5 minutes."
The mental script is this:
- Pause for one breath before responding.
- Consider: “What happens if this waits an hour? A day?”
- Tag it with a quadrant.
- Respond accordingly.
It takes practice. Your instinct will be to react to whoever or whatever is loudest. That’s normal. This model gives your brain a way to sort things so you can make conscious choices instead of getting swept along.
What To Do With Quadrant 3
This is where people get stuck. You’ve identified that something is “urgent-but-not-important.” Now what?
Script for deflecting Quadrant 3:
- “I can help with that. Let me circle back this afternoon once I finish morning sessions.”
- “This sounds important to you. Can you send me the details in an email so I can give it more attention after I wrap up with this patient?”
- “I’m not the right person for this, but [Name] handles equipment issues. Have you connected with them?”
The key: Acknowledge without absorbing. You’re not ignoring people. Really—and, rather—you’re protecting your capacity to do your actual job well.
If your workplace culture genuinely penalizes boundary-setting, that’s a different problem. Prioritization alone won’t fix this. You may be working in a systemically under-resourced or dysfunctional environment. The Eisenhower model helps you see that clearly, which is valuable information even if you can’t immediately change it.
Protecting Quadrant 2
The test of whether you’re using this model well is simple: Are you protecting Quadrant 2 time?
If you’re not scheduling planning time, proactive check-ins, or professional development, your Quadrant 1 will keep expanding. Block Quadrant 2 time on your calendar the way you’d block patient appointments. Treat it as non-negotiable.
What This Model Can't Fix
Let’s be clear: This framework assumes that you have some degree of control over your schedule and boundaries. If you’re being monitored for productivity metrics, if setting boundaries leads to retaliation, if you’re in a workplace that systematically undervalues your time, then prioritization alone won’t solve any of those problems.
The Eisenhower model helps you see the problem clearly. It shows you when the issue is your sorting versus a genuinely unsustainable workload. Both are real. Both matter. But they require different solutions.
If you’re using this model consistently and you’re still drowning, that’s data. It may be time to advocate for systemic changes, renegotiate your role, or consider whether your current position is sustainable long-term.
Why This Matters
Chronic task switching and cognitive overload don’t just make you tired—they impair judgment, drain emotional regulation, and accelerate burnout (Maslach & Leiter, 2016; Weigl et al., 2012). The constant jumping between tasks, the interruptions that knock you off track, or the never-ending sense that you should already be doing something else is what wears people down.
A simple model like this gives your brain a place to set things down. Instead of reacting to whatever shows up first, you have a quick way to pause, sort, and decide what truly needs your attention in that moment.
Over time, many clinicians using this model notice that they feel less scattered and less reactive to interruptions. They begin to trust their decisions more—even on busy days. The work is still demanding, and the hats do not disappear, but there’s a little more space between them.
And in a job that asks so much, that space matters.
ASHA Resources
American Speech-Language-Hearing Association. (n.d.). Ready, set, go! Leadership and precepting in medical settings: Tips for success. ASHA Career Portal. https://careers.asha.org/leadership-and-supervision/ready-set-go-leadership-and-precepting-in-medical-settings-tips-for-success/
American Speech-Language-Hearing Association. (n.d.). Time management: Find more hours in the day. ASHA Career Portal. https://careers.asha.org/on-the-job/time-management-find-more-hours-in-the-day/
American Speech-Language-Hearing Association. (2024). Schools survey report: SLP caseload and workload characteristics trends, 2004–2024. https://www.asha.org/research/memberdata/schools-survey/
Dermer, K. (n.d.). The infinite workday: How to actually leave work at work. American Speech-Language-Hearing Association Career Portal. https://careers.asha.org/on-the-job/the-infinite-workday-how-to-leave-work-at-work/
References
Baethge, A., & Rigotti, T. (2013). Interruptions to workflow: Their relationship with irritation and satisfaction with performance, and the mediating roles of time pressure and mental demands. Work & Stress, 27(1), 43–63. https://doi.org/10.1080/02678373.2013.761783
Covey, S. R. (1989). The 7 habits of highly effective people. Free Press.
Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. https://doi.org/10.1002/wps.20311
Rivera-Rodriguez, A. J., & Karsh, B. T. (2010). Interruptions and distractions in healthcare: Review and reappraisal. Quality & Safety in Health Care, 19(4), 304–312. https://doi.org/10.1136/qshc.2009.033282
Weigl, M., Müller, A., Vincent, C., Angerer, P., & Sevdalis, N. (2012). The association of workflow interruptions and hospital doctors’ workload: A prospective observational study. BMJ Quality & Safety, 21(5), 399–407. https://doi.org/10.1136/bmjqs-2011-000188
Author Bio
Amy Badstubner, AuD, CPC, is a certified career and leadership coach, audiologist, and co-founder of dB Coaching Group. With more than 20 years of experience in health care, business, and coaching, she supports professionals and teams in navigating change, improving communication, and creating momentum without burnout. She has presented nationally, written numerous articles, and been featured on multiple podcasts.